RIVIAM Digital Care’s Hospital Discharge service: ready for NHSE’s Care Traffic Control Centre roll out
Benefits
- Improves patient care and prevents readmission.
- Frees up hospital beds.
- Utilises community and voluntary sector capacity.
- Increases team productivity with data driven decision making and clearer communication.
- Delivers integrated care.
- Greater system wide efficiency.
Fast tracking discharge of medically fit patients
In 2023, RIVIAM introduced its Hospital Discharge service which is currently being rolled out at the Royal United Hospitals Bath NHS Foundation Trust (RUH) to fast-track patient hospital discharge.
The service enables RUH ward teams to make patient referrals simultaneously to multiple community, housing and voluntary sector services working together using RIVIAM at the Community Wellbeing Hub (CWH) in Bath and North East Somerset [1]. Staff at the RUH can then see the status of the care in real time via RIVIAM’s Care Control Dashboard. NHS England plans to expand such Care Traffic Control Centres across England to boost capacity and improve patient flow [2]. RIVIAM’s Hospital Discharge service is a ready-made digital solution to support this ambition.
[1] The CWH uses RIVIAM's Multi-agency Referral Hub service to receive and manage referrals in Bath and North East Somerset for 20 social care, community, housing and voluntary sector organisations.

〝The biggest challenges faced by colleagues working in the hospital is knowing what is available within the community, how to access that support and how to be assured that support is in place. The historical approach of multiple phone calls and referral forms is no longer tenable; we needed to make best use of the technology available to us to simplify the process〞
The challenge
According to NHS England, there are “more than 12,000 patients every day in hospital despite being medically fit for discharge.” [3] Data from The King’s Fund also suggests that discharge delays in England increased throughout 2022 and that the cost of delays in 2022/2023 was at least £1.7 billion, at a time when the NHS is pushing to find cost savings. [4] For patients, being stuck in hospital when they are fit enough to leave is also upsetting.
One of the challenges with reducing delayed discharges is how to access capacity in the care system provided by social care, community, housing and voluntary sector organisations. To make and coordinate discharge dependent referrals to these services often means multiple different referral routes and phone calls – this takes time that hinders patient flow and could be better spent delivering care.
For community, housing and voluntary sector services receiving referrals, it’s hard to access the latest patient information and to co-ordinate referrals for the best follow up care.
RIVIAM's solution
With RIVIAM’s Hospital Discharge service, ward teams at the RUH complete an Onward Admission Referral form giving them one place to refer a patient to a wide range of available community, housing and voluntary sector services at the CWH. This includes commissioned discharge dependent services which cross local authority boundaries.
Immediately reducing admin burden, the referral process is quick and seamless. RIVIAM also auto checks the patient’s details against the NHS Spine Mini service ensuring a high level of data accuracy is captured during the referral process.
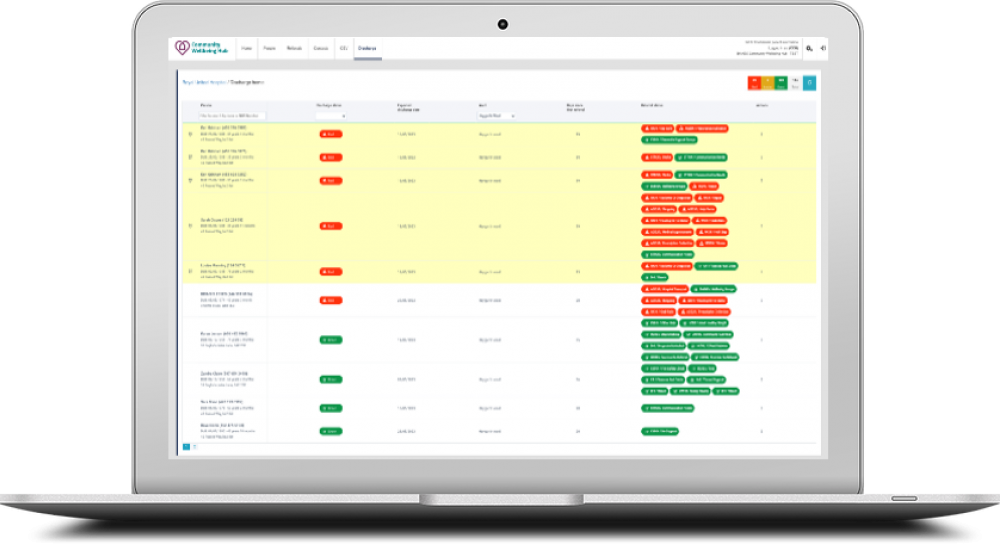
Ward teams then use a Care Control Dashboard to see in real time what’s happening regarding the care they have requested for a person. Status updates and useful information are easily accessible. Online communication reduces the need for phone calls and emails which introduce time delays to a patient’s discharge.
A view of the dashboard is also available for the 20 different partners at the CWH so staff can easily see the person’s most recent ward, their expected discharge date and the different services requested.
Integration with the hospital’s Electronic Health Record (EHR), Cerner Millennium®, means that the dashboard data is seamlessly updated in near real time providing timely visibility of this critical information.
For CWH partners, RIVIAM makes it easy to co-ordinate care for a person with each other, reducing duplication, providing efficiencies, and improving the person’s experience.
〝The impact of this digital transformation is plain to see. For ward staff, the ability to easily make referrals to multiple organisations at the click of a button is revolutionary. However, the ability for Discharge Co-ordinators to then easily see when support has been put in place gives much more assurance that a person can return home safely. This platform is not just a tool; it’s a conduit for change, enabling us to reach those who need us most, right when they need us.〞
〝For the first time, third sector partners can access a dashboard for patients receiving community services to help them join up and co-ordinate care. The dashboard also provides a live data feed from the hospital sharing information about a patient’s status so that the services can be put in place at the right time. The system is transformational.〞
Benefits
- Improves patient care and prevents readmission. People leave hospital as soon as they are medically fit with the right support in place.
- Frees up beds. Patient flow of those who are Clinically Ready for Discharge is improved, relieving pressure on hospital beds.
- Utilises community and voluntary sector capacity. People can recover from a hospital visit at home, with access to local services.
- Increases team productivity through data-driven decision making. There is one place for ward staff to see the latest information about the community care lined up for a person, communicate with them more easily and make quick decisions about discharge.
- Delivers integrated care. Health, social care and voluntary sector providers can receive, manage and co-ordinate and care delivery and communicate with hospital ward teams.
- Greater system-wide efficiency. Real time integration with electronic health records (EHR) provides seamless information flows and insights to reduce time delays, duplication and enable improved care.